To Move Forward, You Have To Let Go : Dealing with knotted wire and disrupted stent
Category: Complication, Coronary,
Case: A 51 years old male was admitted with Acute NSTEMI. He had Type II Diabetes, hypertension, and history of ischemic stroke. His renal function was mildly declined (creatinine 1.5, eGFR 48).
He underwent cardiac catheterization on the third day of hospitalization and was found to have triple vessel coronary disease. The left main artery was large and short. There were significant diseases in proximal to distal LAD (70-90% stenosis), proximal and distal LCx (75, 90% stenosis), and also in distal RCA and mid Right PDA lesion.
Video 1a. Significant lesions in proximal to distal LAD, proximal and distal LCx, distal RCA
Video 1b. Significant lesions in proximal to distal LAD, proximal and distal LCx, distal RCA
Video 1c. Significant lesions in proximal to distal LAD, proximal and distal LCx, distal RCA
Video 1d. Significant lesions in proximal to distal LAD, proximal and distal LCx, distal RCA
Patient rejected CABG and asked for PCI to be done immediately. Target vessel was proximal to distal LAD and proximal LCx .
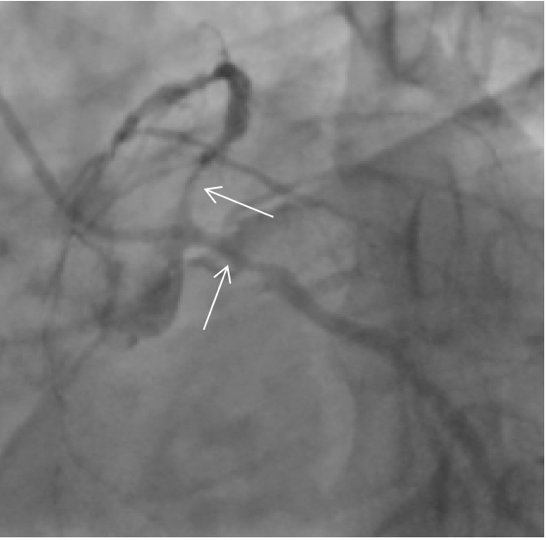

Image 1 A & B: Target vessel for PCI: Proximal LAD, Proximal LCx, Mid-distal LAD
PCI was performed with JL 3.5/6Fr Guide. Workhorse wire was inserted to distal LAD and LCx. First DES (2.5x38 mm) was implanted in mid-distal LAD, with distal stent edge located in D3 bifurcation. Second DES (2.75x24 mm) was implanted in osteal to mid LAD (non overlapping). Proximal stent was post dilated with (3.5x15 mm) NC Balloon.
Video 2a. First stent placement in mid-distal LAD
Video 2b. Second stent placement in osteal-proximal LAD
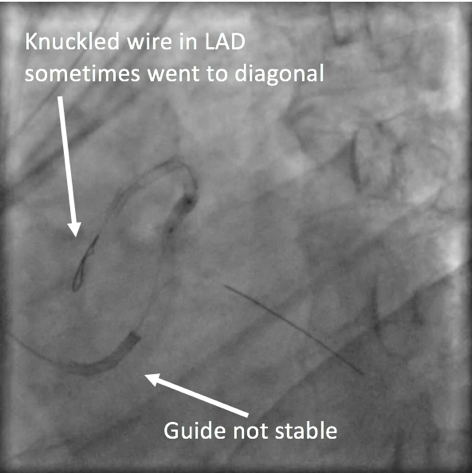
While performing post dilation guide catheter was very unstable. Distal LAD wire was noticed to be knuckled, and sometimes went to D3 branch. Wire felt heavy on reposition attempt. Checking on cranial position, stent was retracted from its original position and distorted.
.png)
Image 2 A - B: Knuckled wire in distal LAD sometimes went to D3 because the guide was unstable
Video 3. Distal LAD stent appeared to be retracted and distorted with wire knotted to distal stent position
.png)
Image 3. Compared to original deployment position
Standard maneuvers failed to release the knotted wire. Additional workhorse wire was inserted crossing the disrupted stent to secure distal LAD. Step dilation was performed using 1.0 x 5 mm and 1.2 x 10 mm normal balloons in knotted wire. 3.0 x 15 mm NC Balloon was inflated in proximal part of disrupted stent (To add more grip).
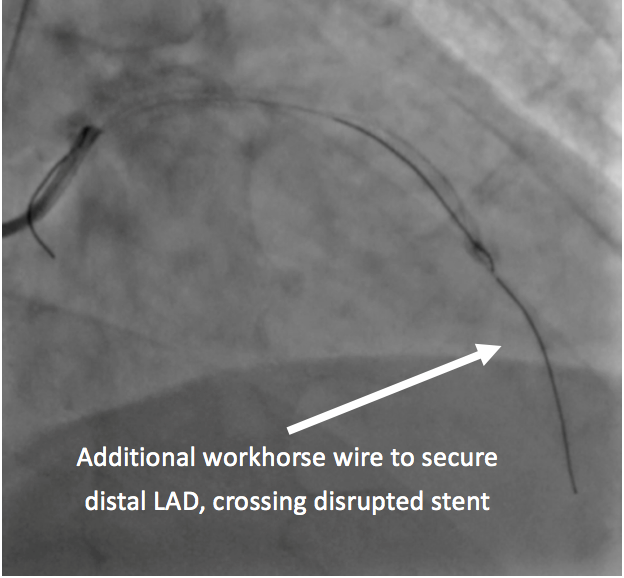
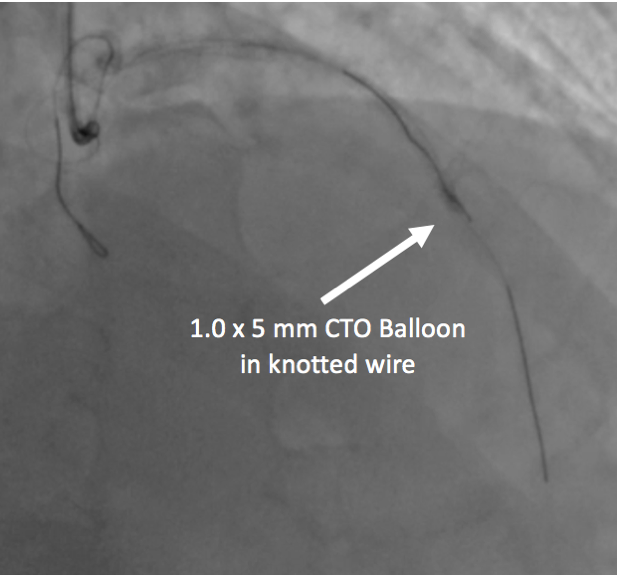
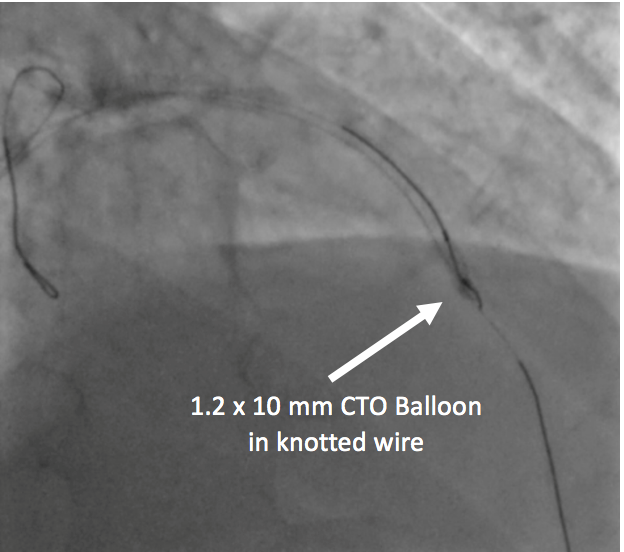
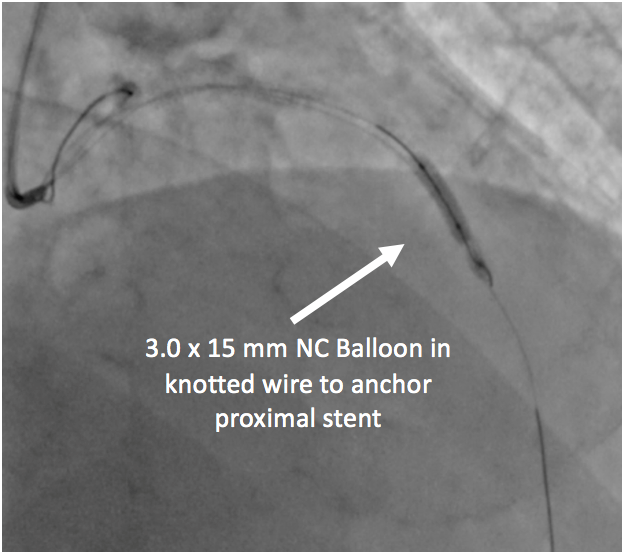
Image 4 A - D: Protecting distal LAD with additional wire and step dilation in knotted wire using small CTO balloons. NC 3.0 balloon was used to add more grip to proximal stent
After dilation, wire was able to be released by using this technique: Loosen the knotted wire, keep turning the wire in one direction (clock / counterclock) – the wire de-knotted by itself. This technique was suggested to the operator by the scrub nurse (A Senior lady, her hobby was knitting).
Video 4. Pulling will only make the knot tighter. Do not do this
Video 5. In this case, De-tensioning the wire while keep rotating in one direction allowed the knot to release itself
Next step is dealing with a disrupted stent. Step dilation was performed through new wire using 1.0 x 5 mm, 1.2 x 10 mm, and 2.0x20 mm normal balloons, crossing disrupted stent struts.
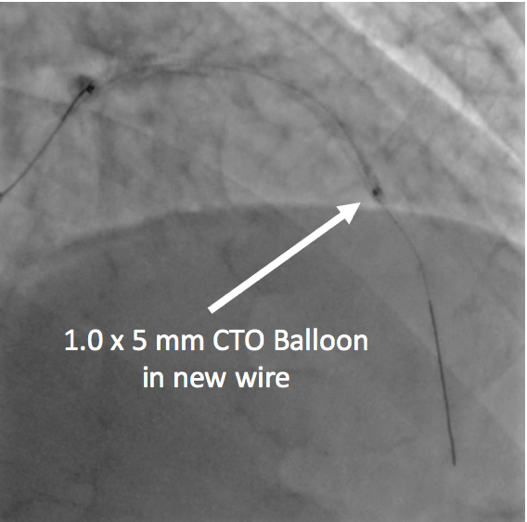

Image 5 A – B: Step dilation in new wire across disrupted stent
2.25x24 mm DES was able to cross disrupted stent and inflated. This stent was then inflated with a 3.5x15 mm NC balloon. Final 3.0 x 28 mm DES was implanted in proximal LCx. Final angiography showed TIMI 3 flow to distal LAD and distal LCx.
Video 6a. A 2.0x20 mm balloon was able to cross disrupted stent struts, followed by 2.25x24 mm DES and postdilated with 3.5 NC Balloon
Video 6b. A 2.0x20 mm balloon was able to cross disrupted stent struts, followed by 2.25x24 mm DES and postdilated with 3.5 NC Balloon
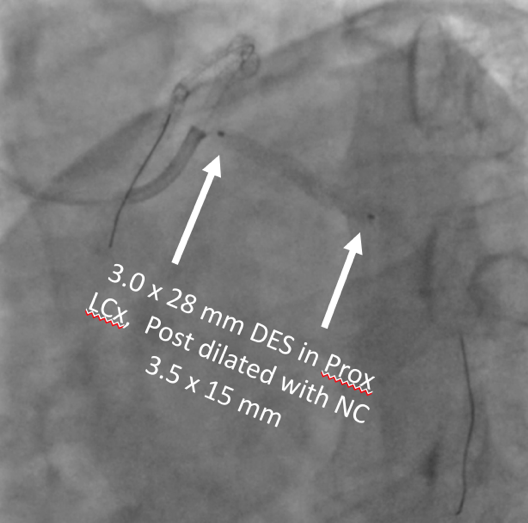
Image 6. Last DES implanted in proximal LCx
Video 7a. Final Angiography
Video 7b. Final Angiography
.png)
Image 7. Procedure Summary: Knotted wire was pulled and caused stent disruption. New wire was put across disrupted stent to protect distal access. After knotted wire successfully retracted, new stent was able to cross disrupted stent and deployed
Discussion and learning points:
This is a complication case caused by several factors: Short LM, unstable guide, stenting in mid bifurcation, knuckled wire, and probably not good enough wire handling. One important lesson in dealing with a wire knot is: Loosen, don't pull. We can try to use small balloon to open more space – after that, keep rotating in one direction and hopefully the wire will untie by itself.
Newer generation stents have more thin strut, which likely more prone to disruption. But it also makes stenting over disrupted stent possible - after a proper step dilation. To avoid knotted wire complication like this case: Never underestimate a knuckled wire tip – especially in a stented lesion.
What I will probably do next time in similar situation: Use a more stable guide, not putting stent in the middle of bifurcation, and be more careful with guidewire handling.
Author's Note:
Operator consulted to Sunarya Soerianata, MD and Doni Firman, MD when performing this case
