Catheter Kinking and Entrapment in Congenital Heart Catheterization: Retrieval Using Snaring Technique
Category: Structural, Congenital, Complication,
INTRODUCTION
Cardiac catheterization has become the gold standard to diagnose and evaluate several complex cardiac abnormalities. The femoral access approach is the commonly used vascular access to perform both of diagnostic and interventional procedures in congenital heart disease. Hematoma, pseudoaneurysm, and retroperitoneal hemorrhage are the most frequent complications following the vascular access from femoral, with reported incidence 2-6%. Kinked catheter during transfemoral access is very rare. We are reporting a case of kinked catheter and entrapment during cardiac catheterization with transfemoral access in patient with complex congenital heart disease.
CASE
A 9-months-old baby boy was diagnosed with double outlet left ventricular, ventricular septal defect, malposed GA, patent ductus arteriosus, pulmonary hypertension, and mild mitral regurgitation caused by AML prolapse.
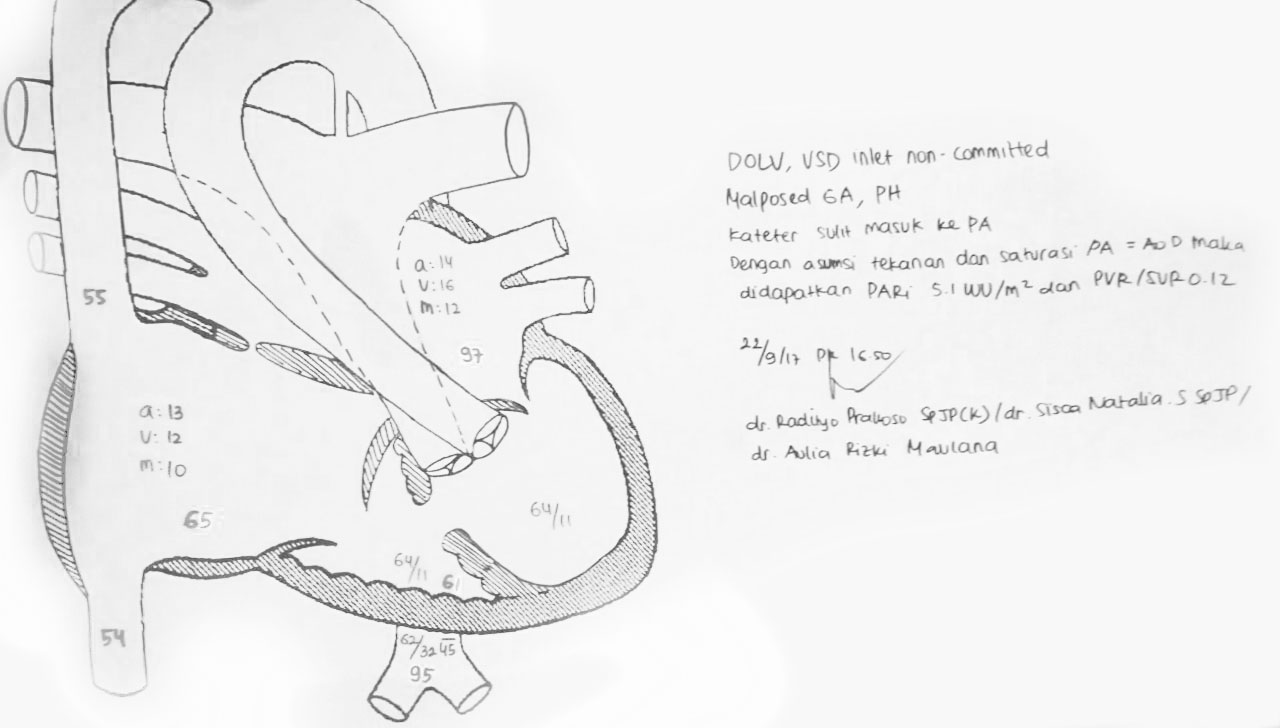
Figure 1. Patient's Heart Anatomy
Cardiac catheterization was performed to evaluate the abnormality of his cardiac through femoral access. After performing the right heart catheterization, we tried to advance a 4F pigtail catheter from right femoral artery (FEAR) to right ventricle (RV) but failed. So, we exchanged a 4F pigtail catheter with a 3.5/4F JR catheter. We also inserted J tipped wire 0.035’’ into a 3.5/4F JR catheter for better maneuver to advance the catheter to the right ventricle. However, while trying to pull and manipulate the guidewire, arterial wave pressure was damped, parallel with inability to further manipulate the catheter. On fluoroscopy, the 3.5/4F JR catheter was found to be kinked at 2 points in the ascending aorta and aortic arch segment.
Video 1. Kinked Catheter
Different maneuvers failed to release the kinked catheter; counterclockwise rotation failed to deloop, and no wires could cross the kinked segment. We decided to use snaring technique from contralateral side (right femoral vein). Another 3.5/4F JR catheter was inserted from right femoral vein to inferior vena cava (IVC), right atrium (RA), right ventricle (RV) and along with 0.035” Terumo wire, The JR catheter entered ascending aorta, aortic arch and descending aorta. The Terumo wire was then replaced with 0.035” Amplatzer wire. Sheath in FEVR was upsized to 6Fr. After that, JR catheter was able to be pulled, and exchanged with a 6F MP (Multipurpose) catheter. Amplatzer wire was used to place a 6F MP catheter in the descending aorta. Then the Amplatzer wire was changed with No. 20 SNARE (Via the MP catheter). Under fluoroscopy, we gently snared in descending aorta and pulled the kinked catheter. Unfortunately, due to the kinked segment, the catheter became straight and stiff, thus difficult to be bend across the aortic arch. It always slipped into the subclavian artery. Then, we moved the ‘’lassoed’’ position to more distal tip of JR catheter and simultaneously pulled the kinked catheter into ascending aorta. It smoothly unfolded its kinked while slipping into the RV, hence freeing the catheter (Video 2).
Video 2. Snaring and Release of Kinked Catheter
The MP catheter and snare wire were pulled out. We continued to perform the left heart catheterization and a left ventriculogram. We conclude that the complication such as kinked catheter during cardiac catheterization could be happened. However, with proper percutaneous catheter-based techniques, maneuvers, and manipulations from skilled operator, we might overcome such problem safely. One of the percutaneous-retrieval techniques that we could use is snaring. From our experiences, snaring and releasing the kinked catheter in ventricle are much more easier.
