Feasibility of Left Distal Transradial Access for PCI
Category: Radial Access, Coronary,
Introduction
Left radial access for coronary angiography and intervention have several benefits. However, conventional left radial access leaves the operator in an ergonomically suboptimal position and subject to higher radiation exposure. Left Distal Transradial access (ldTRA) has recently been introduced as a more practical route for coronary access. We aim to report experiences of coronary angiography and interventions in stable and emergency setting, through ldTRA.
Case Description
We did three consecutive cases with ldTRA: The first case is a 56 years old man with stable angina; which revealed to have functional CTO at LAD. The other two cases were PCI to a 47 years old woman with stable angina, and a primary PCI to a 58 years old man with Inferior STEMI. Coronary angiography and stenting were successfully performed in all cases. Hemostasis was obtained within 3 hours in all patients and without any major bleeding encountered.
Video 1. Left distal trans radial access puncture procedure

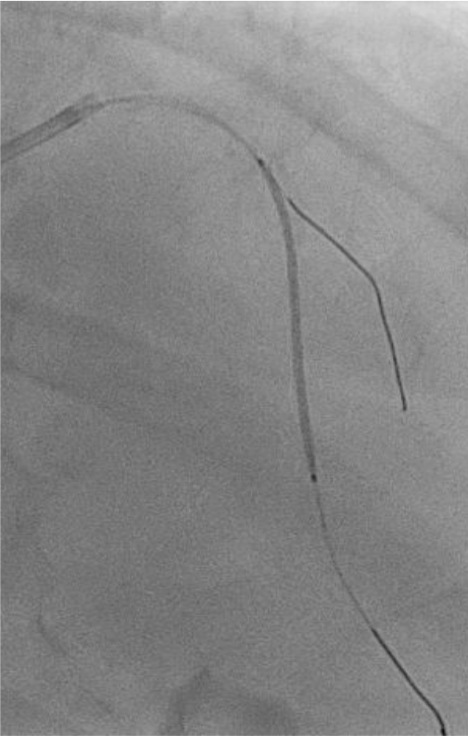


Figure 1. PCI to LAD CTO With 2 Drug Eluting Stents Implanted



Figure 2. Sheath Position, Hemostatic Pressure, Post Hemostatic


Figure 3. Hand Position Before Puncture and Operator Position During Procedure
Discussion and Conclusion
Subclavian artery turtousity is a challenge in coronary angiography and intervention through radial access. This challenge is much less common in left radial, than right. For the right- handed patient, left radial puncture enable free use of the right hand after the procedure. With distal left radial approach, operator could work more comfortable than conventional left radial, especially in obese patient also reduces the chance for radial artery occlusion at the site of the distal forearm. Left distal transradial also perhaps an ideal alternative whenever right radial could not be accessed and we still want to perform transradial access intervention. Further refinement with learning curve will needed to apply this approach smoothly. Left distal transradial access for coronary angiography and intervention is feasible to applied safely in stable and emergency setting. Left distal transradial access could offer several advantages, with patients and operator comfort is also maintained.

The left distal radial artery approach (ldTRA) is an alternative method for patient requiring AV shunt for hemodialysis and for patient on CABG preparation; because there will be no injury to left radial artery. IdTRA can be used as a default technique for patients requiring left over right radial access. However, like TRA, ldTRA requires a learning curve to be mastered. The effective hemostasis method after ldTRA has also not yet been established.
There remains unanswered questions regarding this new technique:
1. How to perform patent hemostasis properly ?
2. Can we use it for second procedure safely ?
3. Should we use routine vascular doppler prior to procedure in patient with weak pulse to confirm accesibility ?